Surry Medical Ministries is a full-service family practice providing integrated primary care with many onsite patient supporting services available. There are two ways (see below) to become a patient at Surry Medical Ministries Health Clinic.
We will accept all NC Medicaid plans serving infants through adults.
Fees for Services:
Any fees for medical, lab or pharmacy services are according to the patient’s Medicaid Provider’s Plan. Please ask our staff if you have any questions! Usual fees are $4 for each medical visit and $4 for most medications.
We do not accept Medicare or Veteran’s Administration health benefits coverage.
At your first visit, please bring: your and/or your children’s Medicaid cards and your photo ID.
You qualify for our services if you meet the following three requirements:
Surry Medical Ministries Clinic focuses on equal access to healthcare for all persons. Our clinic provides primary care services to everyone without regard to race, color, religion, gender, gender expression, national origin, disability, marital status, sexual orientation, military status, or the ability to pay. Fees for referred services are included in all charity care partnership agreements.
It is all financial support a person or each family member receives each month to help pay bills and pay for what the person or family need. This support could be: paychecks, money paid in cash for working, Social Security, Veterans Benefits, Widow’s Benefits, Pensions, a spouse, child or partner’s Disability Income, support for paying rent or utilities from another person or organization. Please ask Surry Medical Ministries staff if you have any questions. We are happy to help!
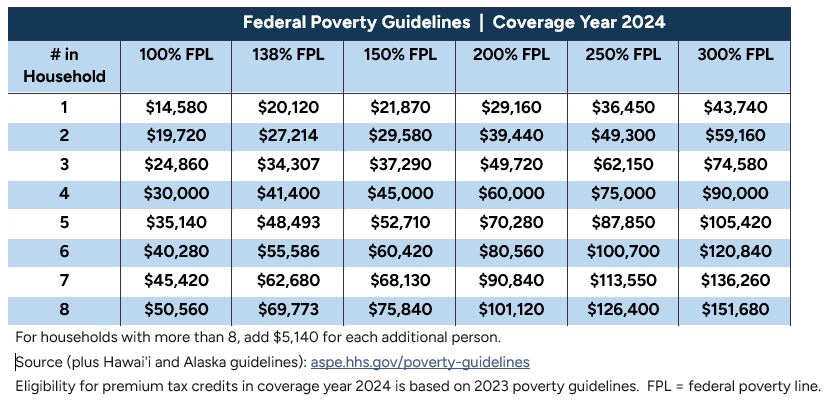
*The limits shown above are based on the 2023 Federal Poverty Guidelines extended by the Department of Health and Human Services
LAB ORDERS – Most Lab orders are $5 or $10 depending on the type.
No patient will be denied services due to an inability to pay.
Uninsured Patients with proof of residence in the Healthcare Partnership Service Area (listed below) may be included in the Charity Care agreement for referral services with Northern Regional Hospital depending on income level and recommended healthcare needed.
NC ZIP CODES – 27030, 27017, 27024, 27041, 27047, 28676, 27053, 27043, 27031, 27045, 27049
VA ZIP CODES – 24317, 24053, 24333, 24328, 24343, 24351, 24352, 24381, 24120, 24177
Note: If you live outside of these zip code areas, Surry Medical Ministries Clinic offers assistance with making a referral and with the completion of qualifying financial assistance applications for any recommended services not offered at our clinic.
HOURS
Mon 9am-5pm
Tue 9am-8pm
Wed 9am-5pm
Thu 9am-5pm
Fri-Sun CLOSED